Anaesthetic use – Study Design
Interventions
Lignocaine injection on one side of the mouth
Saline injection on the other side
Variables measured
Immediate post-surgery
Level of pain during surgery on each side
3 hours post-surgery
- Current level of pain on each side
- Patient’s guess of side injected with lignocaine
- Most comfortable side in 3 hours post-surgery
Statistician’s description of the design
The study was a randomised controlled trial that compared the effects of lignocaine and saline injections on the level of pain reported during and after upper molar surgery. Patients acted as their own controls; each patient had upper molars on both sides removed but received a different palatal injection on each side. The study was double blind as neither the dentist or the patient knew which side received lignocaine.
Calculating the sample size for the study
The study was an equivalence trial; the aim was to show that the average pain levels experienced with or without a palatal injection were equivalent. The differences between the treatments were expected to be small, and must be estimated with good accuracy. The sample size calculations were based on a confidence interval for the mean difference between the two treatments.
“The relevance of the confidence interval … is easier to see. This defines a range for the possible true differences between the treatments, any point of which is reasonably compatible with the observed data. If every point within this range corresponds to a difference of no clinical importance then the treatments may be considered to be equivalent.” (Jones, Jarvis, Lewis & Ebbutt, 1996).
An estimate of the sample size needed was calculated in the following way:
- The measurements of the level of pain from the Visual Analogue Scale were considered; the scores could range from 0 (no pain at all) to 100 (the worst pain imaginable).
- The differences between treatments on the Visual Analogue Scale were estimated to range between -30 and +30; this implies that the standard deviation of the differences is 10.
- The true mean difference between the treatments is assumed to be zero. An equivalence range for the mean difference between the treatments was defined as -5 to +5; in this range, the differences between the treatments are considered to be clinically negligible. The confidence interval should fall inside this range.
- The level of risk of the confidence interval falling wholly or partly outside the equivalence range was set at 0.2; hence the long-term relative frequency of confidence intervals falling inside the equivalence range was 0.8.
- With the parameters described above:
- population standard deviation of differences = 10
- population mean difference = 0
- equivalence range -5 to +5
- 80% of confidence intervals falling inside the equivalence range in the long run
The sample size required was n = 42 patients.
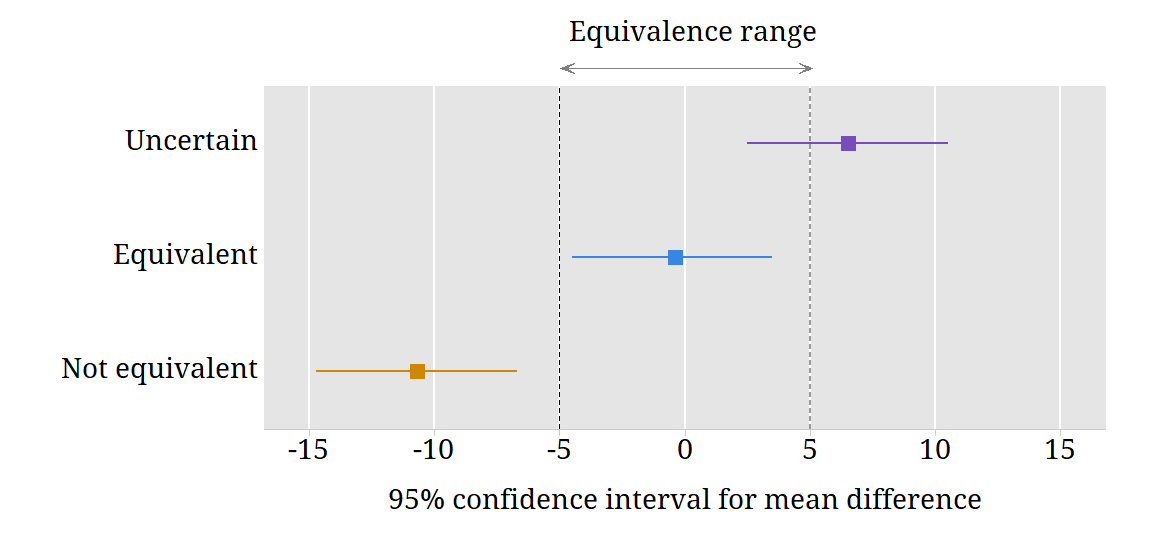
This figure shows the equivalence range for differences between the saline and lignocaine injections. It also shows examples of confidence intervals for this difference. The width of the confidence interval is approximately 4 divided by the square root of sample size.
Randomisation procedure
The planned 50 participants were randomly assigned to receive an injection of lignocaine on either the left side roof or the right side roof of their mouth, and a saline injection on the other side of the roof of their mouth. The random assignment was done in two blocks of 25 patients. Mark planned to analyse the data half way through the trial to see if the outcome was strong enough to stop the trial.
A computer-generated randomisation list was used. Mark Badcock who obtained the list from Randomization.com — a website that generates randomisation lists. The list was sent to the pharmacy staff who prepared the saline and lignocaine solutions for the palatal injections.
Double blinding
Mark Badcock performed all the surgery for the study. For each patient, two vials for the palatal injection were prepared under sterile conditions by the Clinical Trials Department at the Royal Melbourne Hospital Pharmacy. One contained saline and the other lignocaine. The paired vials were labelled “left” and “right” according to the randomisation assigned to that particular patient. When Mark operated on the patient, he did not know which side received lignocaine. The patient also did not know which vial contained lignocaine. However it was possible that during the surgery, the patient may have become aware which side of the roof of his or her mouth felt numb and which did not. It was important that the patient did not tell Mark about this. Mark waited until after the surgery to get any information from the patients about the pain they experienced on both sides of their mouth.
Mark used a computer program to carry out the randomisation. The list of patient numbers and the side on which they received lignocaine was kept by staff in the Clinical Trials Department at the Royal Melbourne Hospital Pharmacy. Mark was only allowed to “break the code” to find out the randomisation at the end of the study, or in some special circumstances described below.
Procedures for meeting ethical concerns
Patients were being asked to undergo a potentially painful procedure without an anaesthetic injection to the roof of the mouth; a dentist would usually give this anaesthetic. A number of procedures were put in place to meet the ethical concerns raised by the study.
Patient withdrawal
Patients were told that they were able to withdraw from the study at any time.
Discontinuing the treatment
If a patient indicated that the pain level was too high, additional (lignocaine) anaesthetic was given, first in the gum and then in the palate if necessary.
Discontinuing the study
If, at any time, five patients required an additional palatal anaesthetic, the allocation of treatments to these patients was examined (before the trial end). If all five additional palatal injections were on the saline side, the trial was to be stopped; if not, then treatment allocation was to be checked for each subsequent patient who needed an additional palatal injection. If, at any time, more than 10% of the patients treated to date needed an additional palatal injection on the saline side, the trial was to be stopped.
No-one who came to the surgery withdrew from the study. No-one needed additional palatal anaesthetic. The study was completed with full participation of all patients.
Mark analysed the data after treating 28 patients. The study was continued; the final sample was 51 patients.
Reference
Jones, B., Jarvis, P., Lewis, J.A., & Ebbutt, A.F. (1996) Trials to assess equivalence: the importance of rigorous methods. British Medical Journal, 313, 36-39.